









Breast agenesis: definitions, causes, diagnosis, treatments and management 
published on 24.10.2025 by Dr Djian
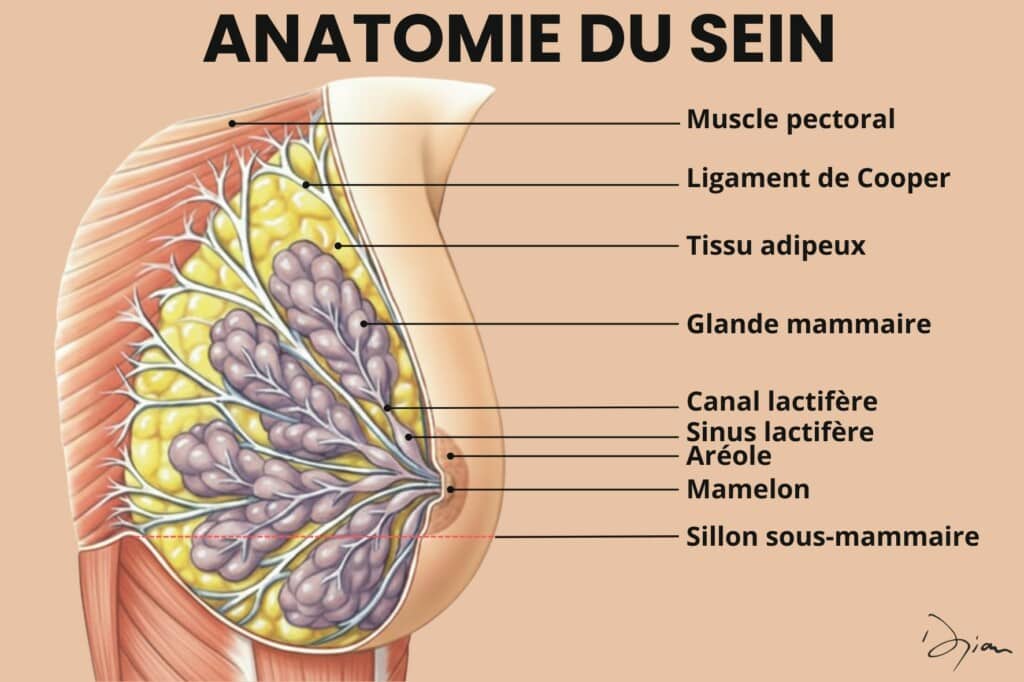
Breast agenesis is the total or partial absence of a mammary gland. Dr. Djian in Paris offers tailor-made solutions for reconstructing natural breasts.


